

CAR T-Cell Therapy & Immune Checkpoint Inhibitors
Two of the most transformative advances in modern oncology are CAR T-Cell Therapy and Immune Checkpoint Inhibitors. Both harness the immune system to fight cancer, but they do so through fundamentally different mechanisms. Checkpoint inhibitors are off-the-shelf antibodies that release the brakes on the immune system, enabling pre-existing T cells to attack tumors. CAR T-cell therapy is a personalized cell therapy where a patient's own T cells are genetically engineered to recognize and kill cancer cells. Checkpoint inhibitors work for many solid tumors; CAR T-cell therapy is primarily for hematologic malignancies. Response to checkpoint inhibitors is often durable in responding patients; CAR T-cell therapy can produce dramatic complete remissions even in patients who have failed multiple prior lines. Toxicity profiles differ: checkpoint inhibitors cause immune-related adverse events affecting any organ; CAR T-cell therapy causes cytokine release syndrome and neurotoxicity. For oncologists, hematologists, and immunologists, the detailed report on CAR T-Cell Therapy provides essential benchmarking data.
H2: Mechanisms Compared
CAR T-Cell Therapy involves genetic modification of autologous T cells. The process: leukapheresis (collecting T cells over 3-5 hours), genetic modification (viral vector transduction or CRISPR editing), expansion (10-14 days in culture), lymphodepletion (chemotherapy to create space for CAR T cells), and infusion (1-3 days after lymphodepletion). The CAR recognizes surface antigen independent of MHC, enabling killing of cancer cells that downregulate MHC (a common immune evasion mechanism). Approved targets: CD19 (B-cell malignancies), BCMA (multiple myeloma). The CAR T cells persist for months to years, providing ongoing surveillance.
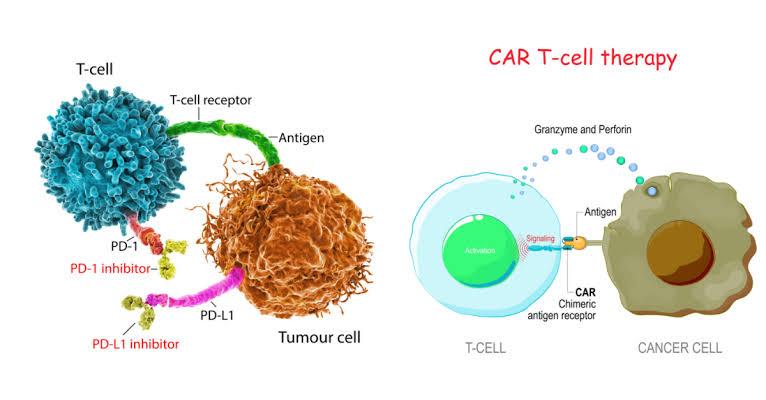
Immune Checkpoint Inhibitors are administered intravenously every 2-6 weeks. No cell collection or modification required. The antibodies block PD-1 (pembrolizumab, nivolumab, cemiplimab), PD-L1 (atezolizumab, avelumab, durvalumab), or CTLA-4 (ipilimumab). These drugs are "off-the-shelf" and can be given immediately. Half-life is 2-4 weeks; treatment typically continues for 2 years or until progression or toxicity. Unlike CAR T cells, checkpoint inhibitors do not persist long-term; the immune response they unleash may persist after drug discontinuation.
H3: Tumor Microenvironment
CAR T-Cell Therapy faces challenges in solid tumors: CAR T cells must traffic to the tumor, infiltrate the stroma, survive in a hostile microenvironment (hypoxia, acidosis, immunosuppressive cytokines), and kill antigen-expressing cells. Tumor heterogeneity (some cells lacking the target antigen) allows escape. These challenges explain why CAR T-cell therapy is less effective in solid tumors. Immune Checkpoint Inhibitors also face resistance mechanisms: upregulation of alternative checkpoints, loss of antigen presentation, and exclusion of T cells from the tumor microenvironment. Combination strategies (checkpoint inhibitors plus chemotherapy, radiation, or other immunotherapies) aim to overcome resistance.
H2: Indications and Patient Selection
CAR T-Cell Therapy is approved for relapsed/refractory B-cell malignancies after at least two prior lines. Patients must have adequate organ function, no active infection, and no uncontrolled autoimmune disease. Tumor must express the target antigen (CD19 or BCMA). Prior allogeneic stem cell transplant is not a contraindication but increases risk of graft-versus-host disease. Age alone is not a contraindication; octogenarians have received CAR T cells.
Immune Checkpoint Inhibitors are approved for first-line and later-line therapy across many cancers. Biomarkers predict response: PD-L1 expression (by immunohistochemistry) for lung cancer, gastric cancer, cervical cancer; tumor mutational burden (high TMB) for multiple cancers; microsatellite instability (MSI-high) or mismatch repair deficiency (dMMR) for any solid tumor. Patients with autoimmune disease are generally excluded from trials but may receive checkpoint inhibitors with caution. Patients with poor performance status (ECOG ≥2) have lower response rates.
H2: Response and Durability
CAR T-Cell Therapy outcomes in DLBCL: complete response (CR) rate 50-60%, overall response (OR) 70-80%. Median progression-free survival (PFS) approximately 6-12 months for non-responders; responders who achieve CR often remain progression-free at 2 years (50-70%). Relapse after CAR T therapy occurs via antigen loss (CD19-negative variants) or CAR T-cell exhaustion. Re-treatment with CAR T cells targeting a different antigen (e.g., CD22 after CD19 relapse) is possible.
Immune Checkpoint Inhibitors outcomes vary by cancer. Melanoma: OR 40-60%, CR 10-15%, median PFS 6-12 months. Lung cancer: OR 20-45%, CR 3-5%, median PFS 4-10 months. Hodgkin lymphoma: OR 70-80%, CR 20-30%, median PFS 12-18 months. Durable responses (ongoing at 5 years) occur in 20-40% of melanoma patients but fewer in other cancers. Patients who achieve CR are likely to remain progression-free; those with partial response or stable disease may eventually progress.
H2: Toxicity Management
CAR T-Cell Therapy toxicities are predictable and manageable. Cytokine release syndrome (CRS): fever (99% of patients), hypotension (50%), hypoxia (30%). CRS grading (1-4) guides management: grade 1 (fever only)—supportive care; grade 2 (hypotension responsive to fluids)—tocilizumab (IL-6 receptor antagonist); grade 3 (hypotension requiring vasopressors)—tocilizumab plus corticosteroids; grade 4—ICU care. Neurotoxicity (ICANS): confusion, aphasia, seizures, cerebral edema. ICANS management: corticosteroids (dexamethasone), supportive care, ICU for severe cases. Long-term toxicities: B-cell aplasia (due to CD19 targeting) requiring immunoglobulin replacement; cytopenias; infections.
Immune Checkpoint Inhibitors toxicities are less predictable and can affect any organ. Dermatologic: rash, pruritus (most common, usually mild). Gastrointestinal: diarrhea, colitis (can be severe, requiring steroids). Hepatic: transaminitis (usually asymptomatic). Pulmonary: pneumonitis (uncommon but potentially fatal). Endocrine: hypophysitis, thyroiditis, adrenalitis (require hormone replacement). Neurologic: myasthenia gravis-like syndrome, encephalitis (rare). Management: grade 1—observation; grade 2—oral corticosteroids; grade 3/4—IV corticosteroids, withhold checkpoint inhibitors, consider infliximab for colitis.
H2: Future Directions
The future of Immune Checkpoint Inhibitors includes novel targets (LAG-3, TIGIT, TIM-3, VISTA), bispecific checkpoint inhibitors (targeting two checkpoints simultaneously), and combination with chemotherapy, radiation, targeted therapy, and other immunotherapies. For CAR T-Cell Therapy, advances include allogeneic (off-the-shelf) CAR T cells, dual-targeting CARs to prevent antigen escape, CARs for solid tumors, and safety switches. For oncologists and hematologists, the market research available on Immune Checkpoint Inhibitors offers comprehensive guidance.